

Sweden Did Not Take Herd Immunity Approach Against Coronavirus Pandemic

There is currently a tsunami of misinformation out there about how Sweden handled the coronavirus pandemic. Sweden did not opt to use a brief hard lockdown like many other countries, but instead put into place a robust set of long-term restrictions that combined both legal bans and voluntary guidelines. This was because leaving a hard lockdown would probably cause a major increase in number of cases as societies opened up again.
The benefits of the Swedish strategy now appears to be confirmed because both the United States and many countries in Europe are now seeing hundreds of post-lockdown outbreaks. The current number of reported cases per day in the United States has passed the previous peak that the brief and hard lockdown was suppose to hammer down and rests on somewhere between 60 000 and 70 000 (which are just the tip of the ice berg as many cases go undiscovered).
In contrast, the number of new reported cases, the number of new ICU cases and the number of deaths are small and continuing going down in July of 2020 in Sweden. During the past 14 days, the average number of new ICU cases for COVID-19 in Sweden was one individual per day according to the Swedish Intensive Care Registry (the featured image above is from this source). More detailed data is presented below. Both deaths and new ICU cases peaked in April.
Sweden did also not go for a herd immunity strategy where the virus burns through the population unhindered. This was rejected as early as March because it would collapse the health care system and the rumor that Sweden relied on a herd immunity strategy came from a Facebook post written by a former employee at the Swedish Public Health Agency that was not involved in the work and a small number of dissident researchs and doctors.
The reason for why there is so much misinformation about Sweden is that the country has been used for decades as a weapon in the domestic political conflicts in the United States about topics such as socialism, universal health care, immigration and feminism. There are powerful forces out there who wants to portray Sweden as a failed state in order to further their own political agenda.
This is true for politicians and newspapers, both conservative and liberal.
Conservatives have wanted to abuse Sweden to argue against using restrictions of any kind. In reality, Sweden did use a robust set of long-term restrictions. Liberals, on the other hand, have attacked Sweden to argue against school openings. In reality, research has shown that leaving primary and lower secondary education open in Sweden made very little difference compared with Finland that closed them down and the idea of school closures had very little support in the literature before the new coronavirus pandemic. However, the situation may well be different in areas with very high social spread (such as the United States in July of 2020) and one should take care not to draw naive generalizations from the data.
Very few journalists and political pundits bothered to go to the source and most preferred to rely on secondhand accounts by scientifically ignorant journalists and political pundits to drive their own political ideology. `
This article goes into the real facts about the Swedish coronavirus strategy with references to the primary data, statements by Swedish public health officials in interviews and press meetings and original documents that are freely available for anyone to check and verify.
What was the Swedish grand strategy against the coronavirus pandemic?
A grand strategy is an overarching strategy that is used to guide individual tactical decisions. The Swedish grand strategy has two main components.
The first component is flattening the curve. The key idea behind this component is that the number of people who need medical attention in a hospital (especially intensive care) should not go above the maximum load of the health care system. This involved banning public gatherings above 50 people, telling people to stay home at the slightest hint of symptoms, shifting high schools and universities to remote education, telling people to work from home if they can, avoiding unnecessary travels, force restaurants and other establishments must create distance between guests and may only serve food at tables, telling people to wash their hands and practice social distancing. National surveys of infection control behaviors, thoughts and feelings among the population has also been carried out continuously to gauge the impact and watch for behavioral trends. Finally, changes in travelling patterns have been monitored nationally via cell phones. There are also multiple national surveillance systems that continue to be active, such as nationally representative panels of people who report symptoms and sentinel surveillance testing.
On the health care side, the number of available ICU beds (fully equipped with supplies and staff) were rapidly scaled up to more than double compared with the national figure before the pandemic. The Swedish Defence Materiel Administration helped with supplies and hospital field tens, while an entire field hospital was built in one week in Älvsjö distinct of Stockholm to further boost available beds. The latter field hospital was later taken down because it was not needed and never used during the peak of cases in Stockholm. The surge capacity for ICU beds have been scaled down as the number of needed ICU beds required have decline to reserve staff capacity, but there has always been around 30% free ICU bed capacity available throughout the pandemic so far, but they are ready to boost the ICU beds against should it be needed.
The second component is protect the elderly. This involved banning visits to elderly care facilities, telling those over 70 to avoid close contacts with other people, online courses in basic health care hygiene and personal protective equipment for staff in health care and elderly care (over 110 000 had taken it within three weeks of being available), boosting testing capacity in health care and elderly care facilities, inspections by the Health and Social Care Inspectorate, cohort care in elderly care facilities and many other improvements.
The Public Health Agency of Sweden has had press meetings every week day through most of the pandemic (recently transitioning into twice per week as cases have gone down) and emphasized this grand strategy over and over. No one can accuse them of communicating poorly since they have literally repeated the same message over and over almost every single weekday.
Where did the myth that Sweden was going for a herd immunity approach come from?
At no point did Sweden adopt a “herd immunity approach”. There is no documents, press conferences or recommendations that show this. It is also disproved by the fact that Sweden did implement many different restrictions, some based on the law and others voluntary. In fact, the Public Health Agency clarified already in March that they were not relying on a herd immunity strategy.

Already on the 15th of March, the Chief epidemiologist in Sweden, Anders Tegnell, said in an interview in Svenska Dagbladet entitled “Tegnell: Flockimmunitet inte huvudtaktiken” (Tegnell: Herd Immunity is not Grand Strategy”) that the tactic in Sweden is not to attain herd immunity by allowing uncontrolled spread:
The main strategy is not about that, but that we have a slow spread of the diseases and that the health care system has a reasonable working environment
In fact, he rejects the idea of herd immunity as a grand strategy as a dangerous experiment:
The current chief epidemiologist has no sympathy for possibly experimenting with disease spread in the society at large, to more rapidly reach herd immunity:
– To experiment with disease spread is a questionable method, says Anders Tegnell.
In a press meeting on May 20, the Swedish chief epidemiologist even pointed out that herd immunity likely cannot even be obtained without a vaccine. This means that it is ludicrous to suggest that the Swedish grand strategy had been herd immunity.
A BBC news item called Did Sweden’s coronavirus strategy succeed or fail?:
Sweden’s authorities never said achieving herd immunity was their goal, but they did argue that by keeping more of society open, Swedes would be more likely to develop a resistance to Covid-19.
So where did this myth come from?
It all started in a Facebook post by the former Chief epidemiologist of Sweden named Annika Linde. But Linde was not involved in the work at all, having retired in 2013. Then this spiraled out of control, got into the media and led to a lot of social media rumors and later adopted by hostile foreign media and a smaller group of dissenting researchers in Sweden. Trump started referencing Sweden as a success because he thought the country had no restrictions. Then he rejected it when disinformation about Sweden started appearing in U.S. media. Liberals have attacked Sweden because they want to keep schools closed and lift Sweden as a horrible example of what happens if you have no lockdown and schools being open.
In reality, political pundits of all parties were wrong on the facts.
Follow Debunking Denialism on Facebook or Twitter for new updates.
What were the results of the Swedish coronavirus strategy?
First, let us look at the national-level data over reported infections, new ICU cases and deaths from the start of the pandemic to late July. The Public Health Agency of Sweden has a statistics dashboard that is similar to the John Hopkins dashboard, but also includes ICU cases. ICU cases are generally considered to be one of the best metrics for how the pandemic is being handled, as the number of reported cases depend on the amount of testing and the number of reported deaths depend heavily on how you report (if people who died at home or died at elderly care facilities are included or excluded, among other methodological issues).
As of July 29 2020, the data looks like this (click to enlarge):

The top graph is the number of reported cases per day. The middle graph is the number of new ICU cases per day and the bottom graph is the number of new deaths per day. There is a lag in death reporting of approximately 7-11 days.
The number of ICU cases and deaths peaked in April. There was always more fully equipped and staffed ICU beds available during the pandemic and the spread did not collapse the health care system.
There is a later peak in the number of reported cases in late June, but this has been shown to be due to increased testing of mild cases that needed no medical assistance. In late May (week 22), there were 36 466 PCR tests carried out per week. This figure jumped to 75 151 in late June (week 26). During weeks 26-28, the number of PCR tests done has varied between about 60 000 and 80 000 tests and between about 50 000 and 65 000 antibody tests done.
Right now, the number of reported cases, the number of new ICU cases and the number of deaths have declined and are down at very, very low levels.
There are weekly reports available from the Public Health Agency of Sweden that goes into additional detail about the global situation, the situation in Sweden, the surveillance systems in Sweden, the number of tests and how many were positive, what proportion of cases that were mild and severe, age and gender distribution, cases in elderly care facilities, geographical distribution, changes in travel patterns, sentinel surveillance in regular outpatient care, intensive care cases and deaths.
The last full week report was published for week 29 that ends in July 24 and is available here. Let us look at a few important graphs from this report.
What about testing?
The Swedish testing strategy involved initial prioritization of patients in the health care system and in elderly care facilities. The second priority was for hospital personell, the third priority was for people with essential jobs and the fourth was any relevant groups. This priority was done because there was an early global limit to the reagents available and tests done should produce a meaningful action. The testing pipeline was later scaled up nationally and now anyone can get tested after some form of medical judgement. Antibody testing is also available.
Here are the number of tests done and their outcomes (click to enlarge):

Light purple is the number of individuals who tested negative and light green is the number of individuals who tested positive. The dark purple is the number of negative tests and dark green is the number of positive tests. The change from individuals to tests in the reporting was done on week 27. This does not include samples from sentinel surveillance. These are available in figure 6 of the same report. In sum, tests are going up and the fraction that are positive is going down.
What about that peak of reported cases in June? Looking closer at the reported cases show that it was almost entirely driven by mild cases that were defined as not needing any medical attention (click to enlarge):

The light green (“Lindriga”) are the mild cases, where as the purlpe (“Allvarliga”) are the severe cases. In case that require any kind of treatment at a hospital is classified as “severe”.
The number of serious cases are in long-term decline and now even the mild cases are going down substantially.
What about elderly care facilities?
Like many countries, the new coronavirus got into the elderly care facilities in Sweden as well and a large fraction of deaths with coronavirus come from these facilities. However, due to influx of resources, personal protective equipment, alcohol gel, guidelines, online education and sharing good practices, the number of new diagnosed cases in elderly care facilities have been rapidly declining (click to enlarge):

Purple is the number of reported cases at elderly care facilities per week. Notice that the number of reported cases is declining even though testing is increasing.
There is broad agreement in Sweden that the country failed with keeping the virus outside elderly care facilities and too many vulnerable elderly individuals died. This has many factors, including cuts to elderly care for decades, each municipality is in charge of their own public and private elderly care facilities and about 40% of staff admitted to not follow basic hygiene routines before the pandemic. Believe it or not, 40% non-compliance is an improvement because it used to be higher.
There is broad variation geographically between regions and within regions on how good they have been at keeping the virus out and suppressing it once it has gotten in. In many regions of Sweden, the virus has never gotten into their facilities in the first place. In others, the spread was stopped at an early phase and yet others completely failed. A lot of lessons will be learned from the differences in how it was handled in elderly care facilities.
What about comparisons to other countries?
Comparing one single metric or a few metrics across many countries (such as the number of reported cases or deaths) is difficult because there are so many confounders that makes the comparison invalid.
The number of reported cases depends on a myriad of factors. The most important factor is how much testing is going on. The number of reported cases is always just the tip of an iceberg of unreported cases, so how much of cases you capture depends crucially on how much you test. Another factor that affects the number of reported cases is where in the pandemic different countries are. Countries that are very early or very late in a pandemic will have fewer reported cases, whereas countries that are in the middle of the pandemic curve will have many. Earlier in the pandemic the diagnostic criteria also differed, with some countries only relying on PCR tests, while some others also included scans of lungs as a diagnostic tool.
The number of reported deaths are also affected by confounders. Some countries did not report deaths in elderly care facilities for a very long time, thereby artificially keeping their figures low. Testing capability also comes in here because a verified death often involve testing for an infection with the new coronavirus. In some countries, many people died at home without any medical attention and these figures are not counted.
Sweden has among the most robust death reporting in the world. This is because in Sweden, it is possible to follow people on the level of personal identification number. Thus, a few times per month, the Public Health Agency of Sweden can search the National Death Registry and pick up people who have died with a COVID-19 diagnosis within the past 30 days. This is almost unique for Sweden and means that our death numbers are a highly accurate representation of reality.
Many other countries do not fully count all of their deaths due to the new coronavirus. A Financial Time report concluded already in April that the global coronavirus death toll could be 60% higher than reported.
What about excess mortality?
So what is the best metric to look at? The best metric to look at is called excess mortality. Simplified, excess mortality means how many more people of different age groups died during 2020 compare with the past few years? This “added deaths” are to a large degree due to the coronavirus pandemic. Not all of them will be, as there are always year-to-year variation in deaths. There is also a risk of underestimating deaths as deaths due to e. g. seasonal influenza has also gone down due to social distancing. But it is the best metric available.
Here is the figure for excess mortality in Sweden during the new coronavirus pandemic (click to enlarge):

Green line is the expected mortality with dashed green lines representing 95% confidence intervals. The purple line is the number of deaths. As can be seen, Sweden experienced excess mortality between week 13 and week 26. Week 27 and onward are considered to have no excess mortality (or more precisely a mortality that is within the normal year-to-year variation).
The European Mortality Monitoring Project has looked closely into excess mortality and Sweden is not the best but far from the worst country. Here is a comparison with a few different countries in Europe (click to enlarge):
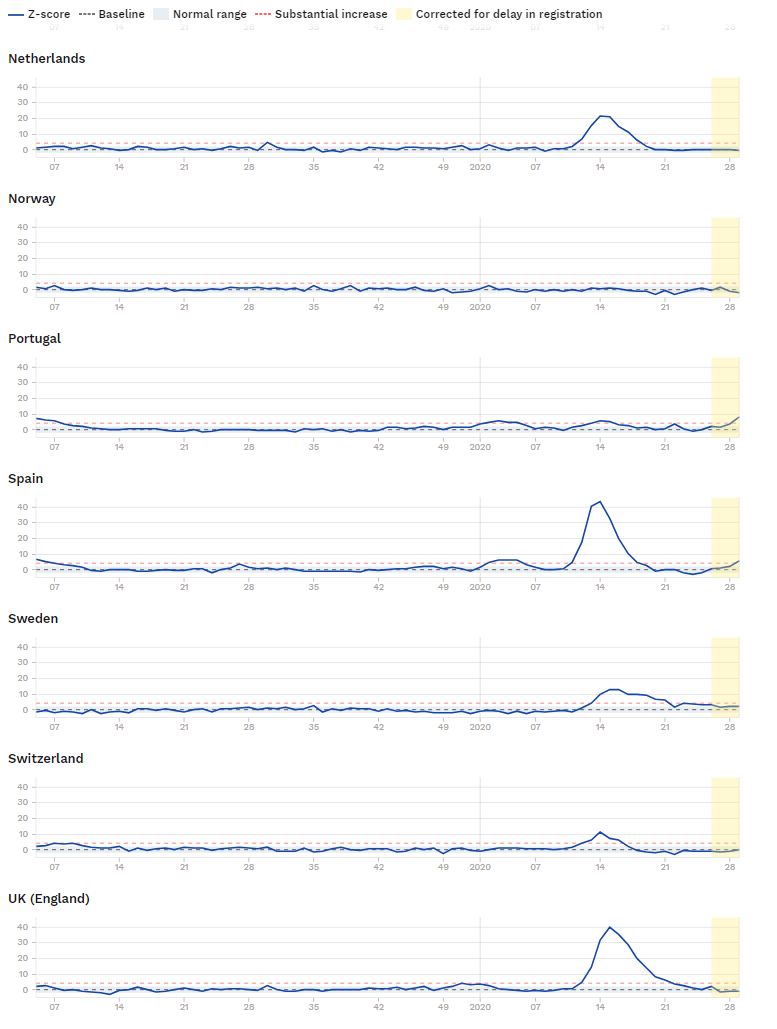
Among the countries European Mortality Monitoring Project looked at, the following countries had about the same or worse excess mortality than Sweden: The United Kingdom, Spain, the Netherlands, Italy, France and Belgium. Several other countries had lower excess mortality than Sweden so far, including Norway, Denmark, Finland and Germany, among others.
How do we know voluntary measures worked?
First of all, Sweden did not only rely on voluntary measures. There were many legal restrictions as well, including maximum 50 participants in public gatherings, bans on visits to elderly care facilities shifting high schools and universities to remote education, restaurants and other establishments must create distance between guests and may only serve food at tables and so on.
Second, we know the voluntary measures were effective because we have seen a decline in the number of reported cases of COVID-19, as well as seasonal influenza and norovirus (vinter-vomiting disease) and finally because people in Sweden has reduced their travelling more than neighboring countries. We have already seen declines in the number of reported cases of COVID-19. Let us look at the standard surveillance for seasonal influenza and norovirus.
The seasonal influenza period peaked in week 10 and ended on week 13. This is the fastest decline that has been observed during the past 20 years in the surveillance for seasonal influenza in Sweden. Here is a graph of the seasonal influenza season during the past few years (click to enlarge):

What about norovirus? The Swedish 2019-2020 season for norovirus ended week 15. Compared with previous years, this is also considerably earlier (click to enlarge):

Green bars are the number of reported lab-confirmed cases for the year 2019-2020, compared with previous years.
Social distancing, increased personal hygiene and so on is an effective method to reduce the spread of both of these diseases. Since their spread collapsed after introducing these measures, we can be confident that they worked.
What about travelling? It is possible to use movement of cell phones to measure the amount of movement and compare it with neighboring countries (click to enlarge):

Not only have people in Sweden traveled much less than they used to, they also traveled less than neighboring countries. This shows that the voluntary recommendation to reduce travelling worked.
What about antibody levels?
Immunity against COVID-19 is not due to just antibodies, but it is known that T cells likely play a large role as well. A recent study from Karolinska Institutet showed that about double the number of people with antibodies had T cell immunity, although much more research is needed to have been done.
Sweden has had a very non-homogeneous spread of the disease with the major epicenter being the capital Stockholm. In late June, about 17.2% of people tested had detectable levels of antibodies in Stockholm in late June. Since antibodies take a few weeks to develop, these reflects infections on or before early June. Since that was two months ago, it is likely that the figure is even higher now. Together with T cell immunity, there appears to be a robust level of immunity in Stockholm.
Earlier national studies on the larger regions found that among people donating blood, the figure was about 6% in late May. Since this is many months ago, the current figures are likely to be much higher.
What about no hard lockdown?
While it is true that Sweden did not use a brief, hard lockdown that prevented people from leaving their homes, there was a robust system of restrictions in place, both legal and voluntary ones, that were designed to be long-term and have been initially set to expire on December 31, 2020. At any time, restrictions can be changed or extended.
This included limiting public gatherings to a maximum of 50 people, banned visits to elderly care facilities, telling people to stay home at the slightest hint of symptoms, shifting high schools and universities to remote education, telling people to work from home if they can, telling those over 70 to avoid close contacts with other people, avoiding unnecessary travels, restaurants and other establishments must create distance between guests and may only serve food at tables, online courses in basic health care hygiene for people in health care and elderly care, substantially increased health care capabilities for testing and so on. Had Sweden gone for a herd immunity strategy as the rumors have it, these restrictions would not have been put in place.
Why did Sweden not use a brief, hard lockdown? This was because it can only be maintained for a short time and there was a substantial risk based on past research that very large outbreaks would happen after the lockdown was lifted. Thus, Sweden decided that it was better to have restrictions that were sustainable and could be maintained for a very long time (such as to the end of the year 2020) to avoid experiencing large resurgences after the lockdown was lifted. There was also a concern that it would be difficult to communicate rapidly changing rules and regulations that go up and down in severity in an understandable way to the population.
As we have seen in recent weeks, there are large resurgences in COVID-19 in many post-lockdown countries, but not in Sweden. Here are just a few newspaper articles in July:
– Coronavirus: Florida sets new state daily case record of 15,299
– Europe braces for second wave of coronavirus
– Catalonia curbs movement of 200,000 people after new coronavirus outbreaks
– Belgium curbs social contact after COVID-19 cases surge
A brief, hard lockdown can be a good idea. But there has to be a coherent and workable post-lockdown plan that needs to be maintained for a long time (more or less the Swedish plan). If not, cases will just rise exponentially again.
Perhaps the best example of this is the United States. They did impose a brief, hard lockdown and are now experiencing a massive resurgence because of failure to plan for life after lockdown. The country will soon pass 150 000 dead. Here is how the John Hopkins dashboard graph looks for newly reported cases:

Will Sweden also see a resurgence after summer? This is very possible, but since there are more who have had the infection in Sweden, the population might be more protected than in some other countries.
Conclusion: Always go to the source
What is the take-home message from all of this?
First, Sweden did not rely on a herd immunity strategy. This is a myth that was spread by social media rumors, former employees who have not been active for almost a decade and a small number of dissenting researchers and doctors. Science employed a robust set of legal and voluntary restrictions and it paid off. The grand strategy was by no means perfect, but it worked to a large degree.
Second, do not trust rumors on social media. Always fact-check them.
Third, do not trust secondary accounts about science and medicine in the media. This even applies media organizations that you trust about other things. Just because a certain newspaper has robust journalism with regards to politics does not mean that they have it with regards to science.
Fourth, always go to the source. Read a wide range of local and regional media. Find the original publications. Look for the data. Ask reputable representatives for the public health system of the countries instead of relying on mavericks.


